
Microtia is a congenital anomaly of external ear (pinna) that ranges from mild structural abnormalities to complete absence of the ear. When an external ear is absent, it is referred to as anotia. Microtia may occur as an isolated deformity although it can also present itself as part of a spectrum of other deformities, either minor or major such as hemifacial microsomia, Goldenhar syndrome and Treacher-Collins syndrome. Most patients with the most severe form of microtia also lack an external auditory canal, also known as “atresia”, that often require treatment for hearing impairment and surgical ear reconstruction.
The reported prevalence of microtia varies among regions, and it is considered to be higher in Hispanics, Asians, Native Americans, and Andeans. The incidence of microtia is reported to be 1 in 8,000 – 10,000 births. Microtia can affect one side only (unilateral) or both sides (bilateral). Microtia occurs more commonly in males and on the right side. Approximately 10 per cent may occur on both sides.

Classification of microtia based on the extent of ear malformation and ear canal damage:
Grade I: Abnormal external small ear with identifiable structures but the external ear canal is present.

Grade II: A partially developed ear (usually the top portion is underdeveloped) with an absence of external ear canal producing a conductive hearing loss.

Grade III: Absence of the external ear with a small peanut-like vestige structure and an absence of the external ear canal and eardrum. Grade III microtia is the most common form of microtia.

Grade IV: Absence of the total ear or anotia. It is the most severe form of microtia and commonly associated with the low-set hairline.

Ideal candidates:
Factors that may influence eligibility for surgery include:
- The severity of external ear deformity
- The extent of hearing loss
- Age (at least 5-6 years old), preferably ten years old or the chest circumference at the level of the xiphoid process is to be at least 60 cm.
- General health
- Motivated and having realistic expectations
Pre-operative evaluation:
The decision to undergo reconstructive ear surgery in a patient with microtia is personal and should be considered appropriately. Before undergoing reconstructive treatment, the surgeon will be working closely with each patient to discuss expectations, preferences, and candidacy for specific procedures.
Not every patient with microtia decides to have reconstructive surgery. Some parents choose to wait and allow their children to decide whether or not to have surgery once they become older. However, younger patients who had successfully undergone ear reconstructive surgery, the majority of them regained a sense of self-confidence, which is essential in the early stage of childhood development.
Reconstructive options for microtia:
The selections of reconstructive option are determined by age, health conditions, patients’ and surgeons’ preferences.
- Prosthetic ear
- Ear reconstruction with synthetic material such as Medpor ear implant
- Autologous reconstruction with rib cartilage (is considered to be the preferred method for microtia reconstruction*)
Description of microtia reconstruction with rib cartilage – using a two-stage technique
A) First stage ear reconstruction
i)Harvesting rib cartilages for ear framework

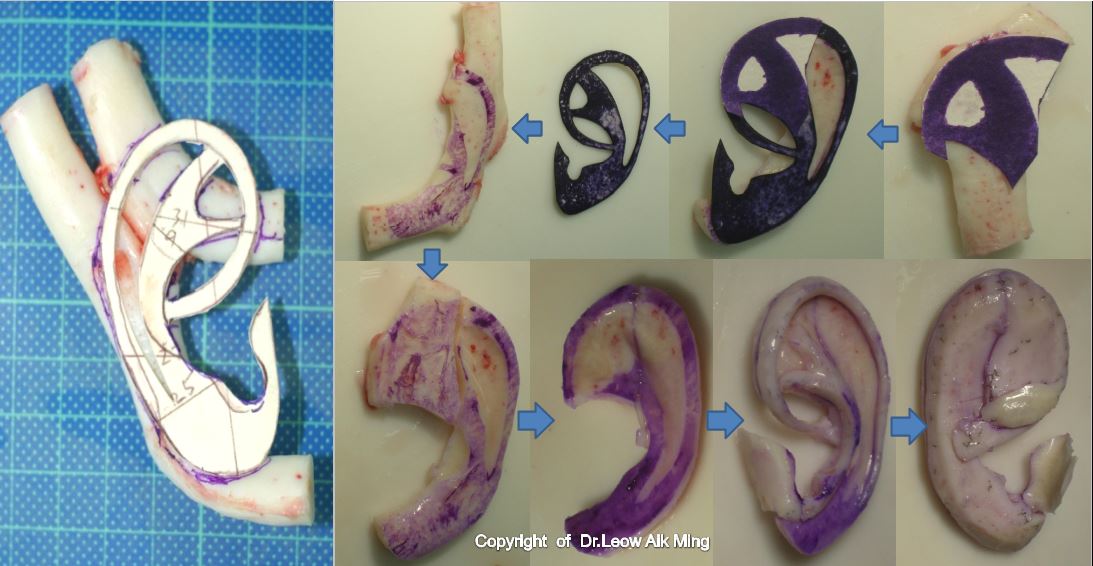
ii) Fabrication of 3-dimensional rib cartilage framework
iii) Creation of pocket, fabrication of skin flap and lobule transposition

iv) Insertion of fabricated ear framework into the skin pocket

B) Second stage ear reconstruction
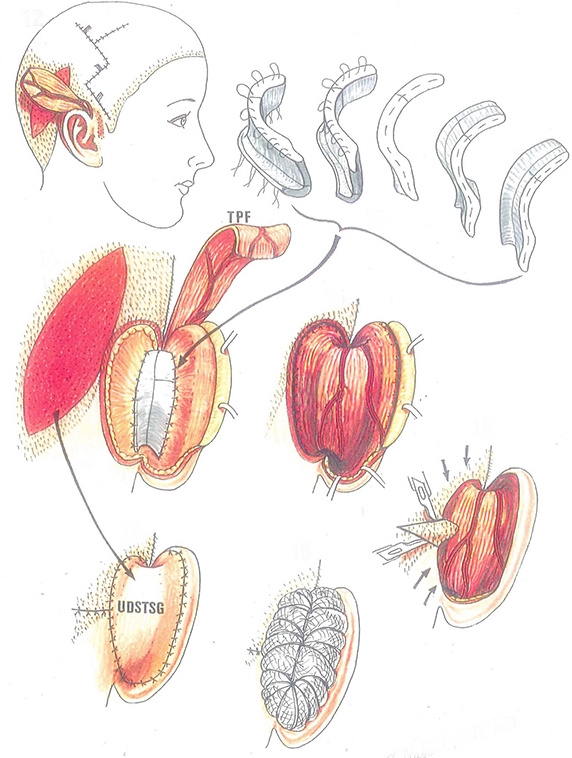
i) Fabrication of cartilage block for the elevation of ear framework

ii) Harvesting fascia flap and skin graft to wrap elevated ear framework

Risks and safety
It is vital for every parents and patient to understand that every surgical procedure has its complications and downtime. However, if a patient is appropriately assessed before the surgery and postoperative care is given adequately, these risks can be eliminated or reduced. The risks involved in ear reconstruction for microtia may vary depending upon the nature of the surgical procedure and complexity. Some of the common risks in surgery include:
- Infection
- Hematoma or seroma
- Skin graft necrosis
- Skin envelop or flap necrosis
- Flap congestion
- Hair loss at the operated site
- Cartilage absorption
- Wire or suture extrusion
- Hypertrophy scar
- Unsatisfactory result
- Asymmetry
- Nerve injury
- Complications from a donor site such as chest wall deformity, pneumothorax and atelectasis
- Risks of general anaesthesia
Post-operative expectations
Reconstructive surgery for microtia of the ear is a complex and challenging surgery. Both parents and patients need to understand the process of recovery and postoperative care to ensure the best surgical outcome. Once the reconstructed ear has completely healed, it will not hinder the patient from any activity and will appear completely normal, resistant to any physical stress or strain.
After the surgery, there will be swelling, bruises, numbness, discomfort and pain at the operated sites. Most of the patients do not experience any significant amount of discomfort at any stages of microtia reconstruction. The degree of discomfort or pain varies from one patient to another. Any form of discomfort or pain after surgery can be easily managed with pain medications. The newly reconstructed ear may not be apparent initially after the surgery due to swelling and bruises. It will usually take about a couple of weeks and months for the shape and landmarks of the ear to be visualised. Ear support or protective dressing should be worn at all time during the initial phase of healing to prevent trauma or excessive pressure to the reconstructed ear. Contact sports should be avoided for 4-6 months.
Post-operative care
- A negative suction drain may be kept for 3-5 days so that the skin can mould to the newly inserted cartilaginous framework
- A soft protective dressing will be applied at all time during the early postoperative period until a review
- Medications will be prescribed such as antibiotics, anti-swelling pills, pain medication and antiseptic solution
- Sutures are to be removed after 7-10 days
- Wound hygiene should be maintained at all time including washing hair regularly
- The patient can participate in light activities with ear protection gear or dressing after 10-14 days
- Contact sports are restricted for about 4 to 6 weeks.
How much will a reconstructive surgery for microtia cost?
Cost is always a consideration in elective surgery. The cost of reconstructive surgery for microtia can vary widely.
The cost of reconstructive surgery for microtia may include:
- Surgeon’s fee
- Hospital or surgical facility costs
- Anaesthesia fees
- Medical tests and
- Prescriptions for medication
In Malaysia, most of the private health insurances do not cover reconstructive surgery for microtia and its related complications.